
Introduction
We’re going to split this article into two parts since the topics within are highly related. The first part will cover training to failure and if it’s important or not for making gains. The second half will focus on a direct byproduct of training to failure – delayed onset muscle soreness, or, DOMS. Strap in, this will be a fun one.
Part I: Training to Failure
“The last three or four reps is what makes the muscle grow. This area of pain divides the champion from someone else who is not a champion. That’s what most people lack, having the guts to go on and just say they’ll go through the pain no matter what happens.” This phrase was uttered by bodybuilding great, Arnold Schwarzenegger, and has been repeated time and time again by many lifters and influencers within the fitness community.
 And really, scientific evidence does show some proof that the muscle is maximally stimulated in the last 3-5 reps of a set leading towards failure (38) – we call these, “stimulating reps” (3). This evidence more than likely stems from a physiological occurrence known as the, “Size Principle.” The Size Principle states that the body will activate smaller motor units first and will call upon larger ones if fatigue develops or if more force is required to move the weight (3,29). Since training to failure induces massive amounts of fatigue, larger motor units must be activated to complete the set which stimulates the entire muscle and, in theory, leads to greater gains.
And really, scientific evidence does show some proof that the muscle is maximally stimulated in the last 3-5 reps of a set leading towards failure (38) – we call these, “stimulating reps” (3). This evidence more than likely stems from a physiological occurrence known as the, “Size Principle.” The Size Principle states that the body will activate smaller motor units first and will call upon larger ones if fatigue develops or if more force is required to move the weight (3,29). Since training to failure induces massive amounts of fatigue, larger motor units must be activated to complete the set which stimulates the entire muscle and, in theory, leads to greater gains.
Several studies have examined the effects of training to failure and many found that failure training is no more effective at inducing muscle hypertrophy than non-failure training (6,9,19,30). Furthermore, studies examined failure training in real-world scenarios and found that multiple sets performed to failure (induced by fatigue from short rest periods) in a workout reduced the total amount of repetitions per set and therefore reduced the overall volume of the workout (39,40,41). We know that workout volume is one of the main keys to inducing hypertrophy (33) so lowering volume is more than likely detrimental to gains. Fewer reps in subsequent sets will also reduce the total amount of mechanical tension experienced by the muscle fibers which can also negatively impact potential gains (3,33).

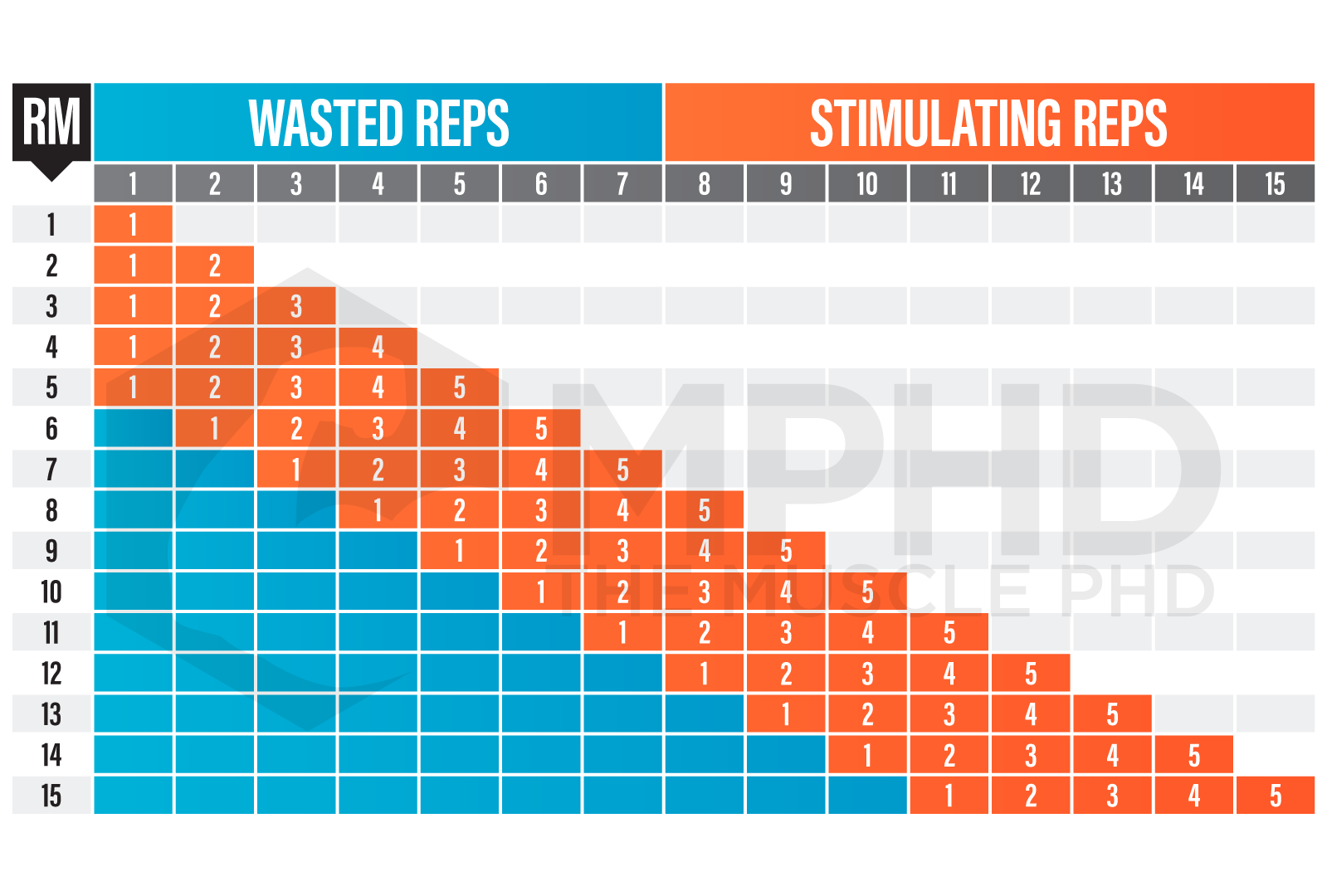
Increasing overall muscle activation is obviously the goal in training to failure, but studies show that maximal muscle activation also occurs when training with heavy loads in excess of 80% 1RM (14,17,21). If we reference the above chart, the muscle is fully activated throughout the entire set at higher intensities which constitutes fewer wasted reps. Perform your “maximally stimulating” 5-reps at 80% + (~8RM+) and you’ll get the same level of activation and number of stimulating reps as you would with training to failure at lighter loads – without having to perform several reps per set.
 Now, the devil’s advocate has its place in every argument and there certainly is some data showing that training to failure may elicit better gains than non-failure training, especially in well-trained individuals (11,27). There is absolutely more evidence to the contrary but it’s worth noting that training to failure may have its place in a training program occasionally and that much of the data we have on hand about failure training was derived from untrained subjects. Untrained populations are obviously going to get benefits from just training in general so training to failure probably won’t offer additional benefits to them. Advanced lifters will more than likely get more benefits out of training to failure.
Now, the devil’s advocate has its place in every argument and there certainly is some data showing that training to failure may elicit better gains than non-failure training, especially in well-trained individuals (11,27). There is absolutely more evidence to the contrary but it’s worth noting that training to failure may have its place in a training program occasionally and that much of the data we have on hand about failure training was derived from untrained subjects. Untrained populations are obviously going to get benefits from just training in general so training to failure probably won’t offer additional benefits to them. Advanced lifters will more than likely get more benefits out of training to failure.
If your goal is to increase the number of stimulating reps in your workout, training to failure is a great way to do that. The downside with that method is that training to failure will greatly increase muscle damage and may make it difficult to hit a muscle group with enough frequency throughout a week to maximally stimulate growth (3). As with most workout methods, use strategies like training to failure as a tool instead of a law. Training to failure can be a small piece of a bigger puzzle, but it’s not the entire puzzle. Reaching failure can be a fun method to mix it up once in a while but the risk: reward ratio and resulting drop in training frequency renders it an unworthy practice to be used consistently. You can train close to failure pretty often and still get a ton of stimulating reps without risking any negative consequences by actually going to failure.
Lastly, training to failure can induce high levels of CNS fatigue, which is likely one reason why we see many protocols struggle to show any benefit with failure training. We get more into this in our CNS Fatigue article here if you’re interested in a more in-depth discussion.

Part II: Delayed Onset Muscle Soreness (DOMS)
If you haven’t heard the phrase, “No pain, no gain,” then you’ve probably been living in a pineapple under the sea. Literally everyone says this. It doesn’t matter if it’s bodybuilding, gymnastics, baseball, or even performing arts, you supposedly have to hurt to get better. We see this ideology all of the time concerning muscle soreness following a workout. If you didn’t get sore, did you even train? Will you even make gains?
 Delayed onset muscle soreness, or DOMS, is the phenomenon that occurs after a brutal training session or after performing novel movements/exercises (22,34). There’s several factors involved that influence the degree of soreness that you feel, but the epicenter of the pain is more than likely due to micro-damage to the muscle fiber and connective tissue and the resulting inflammation response. This damage may sensitize pain receptors within the connective tissue around the muscle which can be further exacerbated by inflammation (7,16,25). This micro-damage may have several causes but one of the easiest explanations is through eccentric muscle actions (8). An eccentric muscle action occurs when the muscle is lengthening, and if you use enough weight or range of motion, this lengthening can cause, “popping,” within the contractile units of the muscle which can disrupt the structural components of the muscle fiber (20). Eccentric muscle actions are a major part of resistance training as you undergo them any time you lower a weight. This is why a heavy training session will produce a ton of DOMS – the muscle will undergo many fatiguing eccentric actions and will also accumulate metabolic byproducts and inflammation that may further contribute to muscle damage (2,25).
Delayed onset muscle soreness, or DOMS, is the phenomenon that occurs after a brutal training session or after performing novel movements/exercises (22,34). There’s several factors involved that influence the degree of soreness that you feel, but the epicenter of the pain is more than likely due to micro-damage to the muscle fiber and connective tissue and the resulting inflammation response. This damage may sensitize pain receptors within the connective tissue around the muscle which can be further exacerbated by inflammation (7,16,25). This micro-damage may have several causes but one of the easiest explanations is through eccentric muscle actions (8). An eccentric muscle action occurs when the muscle is lengthening, and if you use enough weight or range of motion, this lengthening can cause, “popping,” within the contractile units of the muscle which can disrupt the structural components of the muscle fiber (20). Eccentric muscle actions are a major part of resistance training as you undergo them any time you lower a weight. This is why a heavy training session will produce a ton of DOMS – the muscle will undergo many fatiguing eccentric actions and will also accumulate metabolic byproducts and inflammation that may further contribute to muscle damage (2,25).
In addition to sarcomere popping, heavy exercise can also induce excess calcium release which may stimulate enzymes that breakdown muscle proteins and contribute to muscle damage (read here). Explaining muscle damage through the process of eccentrics contractions is much simpler than calcium-induced damage which is why we often only hear one side of the story. However, it’s worth noting that there are multiple contributing factors and we are likely just scratching the surface on findings.
Just for the sake of curiosity, how can we scientifically measure muscle damage? Besides removing subject’s limbs for examination following exercise, a researcher can simply analyze an individual’s blood for markers of muscle damage. As the muscle accrues damage during exercise, the outer wrapping layers of the muscle fibers become more permeable due to the exercise-induced damage. This allows intracellular components of the muscle cell to leak into the blood stream which ultimately elevates levels of creatine kinase (CK) in the blood (2). CK levels are the most commonly measured marker for muscle damage following exercise (2,4).
So is muscle soreness necessary for gains? The classic thought is that you tear down the muscle in the weightroom, and heal/rebuild it which ultimately grows bigger muscles (1,26). It’s important to offer a distinction here, though. Muscle repair and muscle growth are two separate processes – repairing a muscle fiber does not make it larger (2). If muscle repair actually increased the size of a muscle, you could just stab yourself in the thigh and make quad gains – obviously that’s not the case. Muscle fibers can either grow through adding contractile proteins to increase fiber density, or by adding more contractile units in series which increases muscle fiber length (2,33,34). Muscle fibers may also increase in size by increasing intracellular fluid/components through a process known as sarcoplasmic hypertrophy (33) but that would have little to do with muscle damage and is outside the scope of this article.
 We’ll sum it up quickly again: studies have shown that muscle damage is not necessary for growth and does not increase growth compared to subjects with less muscle damage (5,12,15,32). Furthermore, the amount of soreness you experience is poorly correlated to how much muscle damage has actually occurred (23) so the more soreness you experience won’t exactly translate to the degree of muscle damage. In addition, aerobic exercise like jogging can induce high amounts of muscle damage but doesn’t result in growth (5).
We’ll sum it up quickly again: studies have shown that muscle damage is not necessary for growth and does not increase growth compared to subjects with less muscle damage (5,12,15,32). Furthermore, the amount of soreness you experience is poorly correlated to how much muscle damage has actually occurred (23) so the more soreness you experience won’t exactly translate to the degree of muscle damage. In addition, aerobic exercise like jogging can induce high amounts of muscle damage but doesn’t result in growth (5).
Now, time for the devil’s advocate again. Muscle damage does promote inflammation which can promote several different anabolic signals and processes (33,34). Cell inflammation somewhat acts as another component of tension on the muscle fiber – cell swelling stresses the cell membrane which forces the cell to increase protein synthesis signaling and increase in size to lessen the stress (13,18,37). However, muscle damage is not necessary to increase inflammation or cell swelling (42).
Another potential devil’s advocate is the fact that muscle damage may promote satellite cell activity which appears to be necessary for long term growth (10,28,35). Unfortunately for the sore muscles crew, muscle damage is, again, not necessary for increasing satellite cell activation (2,24,34).
Conclusion
Ultimately, muscle soreness is just an aspect of training and should not be the main goal of training. Individuals will experience soreness differently and many people will have certain muscle groups that experience soreness more severely than others (36). For me, my adductors get insanely sore from squats while my quads rarely have any tenderness. Does that mean my quads are not growing? Of course not. You can have gains without the pain, just don’t take this to the extreme too much. You still have to push yourself and place the muscle through high amounts of tension and stress to grow; that will more than likely result in soreness. Extreme muscle damage has actually been shown to be detrimental to gains and progress (31), so don’t follow the hype that gains stem from insane amounts of pain.
We’ll sum the entire article up with the best quote when it comes to training to failure and soreness: “Stimulate; don’t annihilate.” Lee Haney won 8-Mr. Olympia titles with this credo in mind and the science seems to agree. Destroying yourself day in and day out in the weightroom will not offer extra gains and may ultimately be detrimental to your goals. Use training to failure as an occasional tool, and don’t be bummed if you can still walk the day after a leg workout.
References
- Barash, I. A., Mathew, L., Ryan, A. F., Chen, J., & Lieber, R. L. (2004). Rapid muscle-specific gene expression changes after a single bout of eccentric contractions in the mouse. American Journal of Physiology-Cell Physiology, 286(2), C355-C364.
- Beardsley, C. (2018). Does muscle damage cause hypertrophy? Retrieved from: https://medium.com/@SandCResearch/does-muscle-damage-cause-hypertrophy-bf99b652694b
- Beardsley, C. (2018). How does training volume differ between training to failure, avoiding failure, and using advanced techniques? Retrieved from: https://medium.com/@SandCResearch/how-does-training-volume-differ-between-training-to-failure-avoiding-failure-and-using-advanced-90e26d57bca9
- Brancaccio, P., Maffulli, N., & Limongelli, F. M. (2007). Creatine kinase monitoring in sport medicine. British Medical Bulletin, 81(1), 209-230.
- Brentano, M. A., & Martins Kruel, L. F. (2011). A review on strength exercise-induced muscle damage: applications, adaptation mechanisms and limitations. Journal of Sports Medicine & Physical Fitness, 51(1), 1-10.
- Burd, N. A., West, D. W., Staples, A. W., Atherton, P. J., Baker, J. M., Moore, D. R., … & Phillips, S. M. (2010). Low-load high volume resistance exercise stimulates muscle protein synthesis more than high-load low volume resistance exercise in young men. PLOS One, 5(8), e12033.
- Clarkson, P. M., & Hubal, M. J. (2002). Exercise-induced muscle damage in humans. American Journal of Physical Medicine & Rehabilitation, 81(11), S52-S69.
- Cleak, M. J., & Eston, R. G. (1992). Muscle soreness, swelling, stiffness and strength loss after intense eccentric exercise. British Journal of Sports Medicine, 26(4), 267-272.
- Davies, T., Orr, R., Halaki, M., & Hackett, D. (2016). Effect of training leading to repetition failure on muscular strength: a systematic review and meta-analysis. Sports Medicine, 46(4), 487-502.
- Dhawan, J., & Rando, T. A. (2005). Stem cells in postnatal myogenesis: molecular mechanisms of satellite cell quiescence, activation and replenishment. Trends in Cell Biology, 15(12), 666-673.
- Drinkwater, E. J., Lawton, T. W., Lindsell, R. P., Pyne, D. B., Hunt, P. H., & McKenna, M. J. (2005). Training leading to repetition failure enhances bench press strength gains in elite junior athletes. The Journal of Strength & Conditioning Research, 19(2), 382-388.
- Flann, K. L., LaStayo, P. C., McClain, D. A., Hazel, M., & Lindstedt, S. L. (2011). Muscle damage and muscle remodeling: no pain, no gain? Journal of Experimental Biology, 214(4), 674-679.
- Grant, A. C. G., Gow, I. F., Zammit, V. A., & Shennan, D. B. (2000). Regulation of protein synthesis in lactating rat mammary tissue by cell volume. Biochimica et Biophysica Acta (BBA)-General Subjects, 1475(1), 39-46.
- Krieger, J. W. (2010). Single vs. multiple sets of resistance exercise for muscle hypertrophy: a meta-analysis. The Journal of Strength & Conditioning Research, 24(4), 1150-1159.
- LaStayo, P., McDonagh, P., Lipovic, D., Napoles, P., Bartholomew, A., Esser, K., & Lindstedt, S. (2007). Elderly patients and high force resistance exercise—a descriptive report: can an anabolic, muscle growth response occur without muscle damage or inflammation? Journal of Geriatric Physical Therapy, 30(3), 128-134.
- Malm, C. (2001). Exercise‐induced muscle damage and inflammation: fact or fiction? Acta Physiologica Scandinavica, 171(3), 233-239.
- Marshall, P. W., McEwen, M., & Robbins, D. W. (2011). Strength and neuromuscular adaptation following one, four, and eight sets of high intensity resistance exercise in trained males. European Journal of Applied Physiology, 111(12), 3007-3016.
- Millar, I. D., Barber, M. C., Lomax, M. A., Travers, M. T., & Shennan, D. B. (1997). Mammary protein synthesis is acutely regulated by the cellular hydration state. Biochemical and Biophysical Research Communications, 230(2), 351-355.
- Mitchell, C. J., Churchward-Venne, T. A., West, D. W., Burd, N. A., Breen, L., Baker, S. K., & Phillips, S. M. (2012). Resistance exercise load does not determine training-mediated hypertrophic gains in young men. Journal of Applied Physiology, 113(1), 71-77.
- Morgan, D. L., & Proske, U. (2004). Popping sarcomere hypothesis explains stretch‐induced muscle damage. Clinical and Experimental Pharmacology and Physiology, 31(8), 541-545.
- Naclerio, F., Faigenbaum, A. D., Larumbe-Zabala, E., Perez-Bibao, T., Kang, J., Ratamess, N. A., & Triplett, N. T. (2013). Effects of different resistance training volumes on strength and power in team sport athletes. The Journal of Strength & Conditioning Research, 27(7), 1832-1840.
- Nosaka, K. (2011). Exercise-induced muscle damage and delayed onset muscle soreness (DOMS). In: Strength and conditioning: Biological principles and practical applications. Cardinale, M, Newton, R and Nosaka, K, eds. West Sussex, UK: John Wiley and Sons. pp. 187.
- Nosaka, K., Newton, M., & Sacco, P. (2002). Delayed‐onset muscle soreness does not reflect the magnitude of eccentric exercise‐induced muscle damage. Scandinavian Journal of Medicine & Science in Sports, 12(6), 337-346.
- Paulsen, G., Ramer Mikkelsen, U., Raastad, T., & Peake, J. M. (2012). Leucocytes, cytokines and satellite cells: what role do they play in muscle damage and regeneration following eccentric exercise? Exercise Immunology Review, 18, 42-97.
- Proske, U., & Morgan, D. L. (2001). Muscle damage from eccentric exercise: mechanism, mechanical signs, adaptation and clinical applications. The Journal of Physiology, 537(2), 333-345.
- Radak, Z., Chung, H. Y., Koltai, E., Taylor, A. W., & Goto, S. (2008). Exercise, oxidative stress and hormesis. Ageing Research Reviews, 7(1), 34-42.
- Rooney, K. J., Herbert, R. D., & Balnave, R. J. (1994). Fatigue contributes to the strength training stimulus. Medicine and Science in Sports and Exercise, 26(9), 1160-1164.
- Russell, B., Dix, D. J., Haller, D. L., & Jacobs-El, J. (1992). Repair of injured skeletal muscle: a molecular approach. Medicine and Science in Sports and Exercise, 24(2), 189-196.
- Sale, D. G. (1987). Influence of exercise and training on motor unit activation. Exercise and Sport Sciences Reviews, 15, 95-151.
- Sampson, J. A., & Groeller, H. (2016). Is repetition failure critical for the development of muscle hypertrophy and strength? Scandinavian Journal of Medicine & Science in Sports, 26(4), 375-383.
- Sayers, S. P., & Clarkson, P. M. (2001). Force recovery after eccentric exercise in males and females. European Journal of Applied Physiology, 84(1-2), 122-126.
- Schoenfeld, B. J. (2012). Does exercise-induced muscle damage play a role in skeletal muscle hypertrophy? The Journal of Strength & Conditioning Research, 26(5), 1441-1453.
- Schoenfeld, B. J. (2010). The mechanisms of muscle hypertrophy and their application to resistance training. The Journal of Strength & Conditioning Research, 24(10), 2857-2872.
- Schoenfeld, B. J., & Contreras, B. (2013). Is postexercise muscle soreness a valid indicator of muscular adaptations? Strength & Conditioning Journal, 35(5), 16-21.
- Schultz, E., Jaryszak, D. L., & Valliere, C. R. (1985). Response of satellite cells to focal skeletal muscle injury. Muscle & Nerve: Official Journal of the American Association of Electrodiagnostic Medicine, 8(3), 217-222.
- Sikorski, E., et. al. (2013). Changes in perceived recovery status scale following high-volume muscle damaging resistance exercise. The Journal of Strength & Conditioning Research, 27(8), 2079-2085.
- Stoll, B. A., & Secreto, G. (1992). Prenatal influences and breast cancer. Lancet (London, England), 340(8833), 1478.
- Sundstrup, E., Jakobsen, M. D., Andersen, C. H., Zebis, M. K., Mortensen, O. S., & Andersen, L. L. (2012). Muscle activation strategies during strength training with heavy loading vs. repetitions to failure. The Journal of Strength & Conditioning Research, 26(7), 1897-1903.
- Willardson, J. M., & Burkett, L. N. (2005). A comparison of 3 Different Rest Intervals on the Exercise Volume Completed During A Workout. The Journal of Strength & Conditioning Research, 19(1), 23-26.
- Willardson, J. M., & Burkett, L. N. (2006). The effect of rest interval length on bench press performance with heavy vs. light loads. Journal of Strength and Conditioning Research, 20(2), 396.
- Willardson, J. M., & Burkett, L. N. (2006). The effect of rest interval length on the sustainability of squat and bench press repetitions. Journal of Strength and Conditioning Research, 20(2), 400.
- Yu, J. G., Malm, C., & Thornell, L. E. (2002). Eccentric contractions leading to DOMS do not cause loss of desmin nor fibre necrosis in human muscle. Histochemistry and Cell Biology, 118(1), 29-34.
From being a mediocre athlete, to professional powerlifter and strength coach, and now to researcher and writer, Charlie combines education and experience in the effort to help Bridge the Gap Between Science and Application. Charlie performs double duty by being the Content Manager for The Muscle PhD as well as the Director of Human Performance at the Applied Science and Performance Institute in Tampa, FL. To appease the nerds, Charlie is a PhD candidate in Human Performance with a master’s degree in Kinesiology and a bachelor’s degree in Exercise Science. For more alphabet soup, Charlie is also a Certified Strength and Conditioning Specialist (CSCS), an ACSM-certified Exercise Physiologist (ACSM-EP), and a USA Weightlifting-certified performance coach (USAW).